The results of this research were published in Global Advances in Health and Medicine in January 2013.
Study title: Heart Rate Variability Biofeedback in Adolescent Substance Abuse Treatment
Authors: Chris Thurstone, MDcorresponding author and Travis Lajoie, DO
Citation: Glob Adv Health Med. 2013 Jan; 2(1): 22–23
Strategies are needed to improve adolescent substance abuse treatment outcomes. For example, during outpatient substance abuse treatment, up to 80% of adolescents continue to use. Following residential substance abuse treatment, 88% of adolescents relapse within 6 months.
Psychosocial stress plays an important role in the maintenance of substance use and also in relapse. A study of 2031 16- to 24-year-olds with past-month marijuana use showed that 56% used marijuana in the past month to cope with life stress. Furthermore, in a study of 81 adolescents (aged 13–18 years) followed for 6 months after treatment, 67% of those who relapsed reported a stressful event just prior to relapse. Therefore, treatment outcomes might be improved by interventions that help teens cope with stress.
Heart rate variability (HRV) biofeedback may be a good intervention for this population because it reduces stress in adolescents who are not receiving treatment for substance abuse. Furthermore, HRV patterns of low amplitude and coherence are found in adults with substance use disorders during craving states and in youth with disorders (eg, oppositional defiant disorder and conduct disorder) that frequently lead to substance use. HRV biofeedback also reduces mean salivary cortisol levels, and corticotropin-releasing factor inhibitors have been shown to reduce stress-related relapse in animal models.9,10 Despite these findings, there are no controlled studies examining the role of HRV biofeedback to help prevent relapse following substance abuse treatment.
To address this research gap, this case letter evaluates the preliminary feasibility of HRV biofeedback to augment adolescent substance abuse treatment.
The patient is a 17-year-old male who presented to substance treatment for cannabis use. He started smoking marijuana at age 12 and started smoking daily at age 14. Starting at age 14, he had multiple convictions including possession of illicit substances, motor vehicle theft, and reckless driving. Despite being in a juvenile detention center, on ankle monitoring, and on probation for 3 years, he felt “hopeless” and “overwhelmed” about not being able to stop smoking marijuana for more than 4 weeks. Therefore, he voluntarily sought substance treatment. He identified stress and anger as primary triggers for marijuana use.
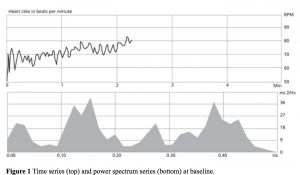 On admission, the patient met Diagnostic and Statistical Manual of Mental Disorders, 4th edition, criteria for cannabis dependence and conduct disorder by clinical interview. He reported daily marijuana use until 4 weeks before baseline. His Perceived Stress Score was 18, with mean scores for males his age being 14.7 (SD = 7.2) The baseline HRV time series plot, shown in Figure 1, showed irregular, jagged waveforms. The baseline power series plot showed signals of various frequency spectra. Both findings suggesting concurrent sympathetic and parasympathetic nervous system input.
On admission, the patient met Diagnostic and Statistical Manual of Mental Disorders, 4th edition, criteria for cannabis dependence and conduct disorder by clinical interview. He reported daily marijuana use until 4 weeks before baseline. His Perceived Stress Score was 18, with mean scores for males his age being 14.7 (SD = 7.2) The baseline HRV time series plot, shown in Figure 1, showed irregular, jagged waveforms. The baseline power series plot showed signals of various frequency spectra. Both findings suggesting concurrent sympathetic and parasympathetic nervous system input.
Over 20 weeks, the patient received nine sessions of individual, manual-standardized cognitive behavioral therapy (CBT) and two family sessions. He also received six 10-minute sessions of HRV biofeedback following his 50-minute CBT sessions. The biofeedback sessions were integrated with the themes of his CBT sessions, which included modules such as coping with cravings, communication skills, anger management, and problem solving. The biofeedback sessions used emWave Desktop Stress Relief (HeartMath, LLC, Boulder Creek, California) and were conducted by a certified HeartMath practitioner.
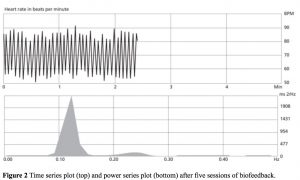 The patient reported no substance use during treatment and provided a negative urine drug screen at each treatment visit. The HRV tracings, shown in Figure 2, showed improved amplitude and coherence, suggestive of increased parasympathetic nervous system input.5 At the end of treatment, the patient’s Perceived Stress Scale was 5, which was consistent with the patient reporting feeling “calmer” and “more confident.” The patient reported using the biofeedback techniques regularly during stressful moments and prior to athletic events. His grade point average increased from a 1.6 to a 3.1 on a 4-point scale. In a follow-up telephone call 1 year after treatment, the patient reported continued sobriety and that he uses the biofeedback techniques daily. He is currently enrolled in a 4-year university.
The patient reported no substance use during treatment and provided a negative urine drug screen at each treatment visit. The HRV tracings, shown in Figure 2, showed improved amplitude and coherence, suggestive of increased parasympathetic nervous system input.5 At the end of treatment, the patient’s Perceived Stress Scale was 5, which was consistent with the patient reporting feeling “calmer” and “more confident.” The patient reported using the biofeedback techniques regularly during stressful moments and prior to athletic events. His grade point average increased from a 1.6 to a 3.1 on a 4-point scale. In a follow-up telephone call 1 year after treatment, the patient reported continued sobriety and that he uses the biofeedback techniques daily. He is currently enrolled in a 4-year university.
In summary, this case shows promise for HRV biofeedback to augment individual CBT for adolescent substance treatment. Future studies should evaluate the efficacy of a manual-standardized HRV biofeedback intervention using a control group.

We welcome all thoughtful comments, but please abide by our commenting rules